
The FDA’s “Smoking Gun” V-Safety Slide From October 2020
Originally published on Trial Site News.
On August 23, 2021, the US Food and Drug Administration (FDA) granted approval (or licensure) to the first ever COVID-19 mRNA gene therapy product by Pfizer/BioNTech, which from the onset was misbranded as a ‘vaccine.’
The Acting FDA Commissioner Janet Woodcock, M.D., said at the time: “The FDA’s approval of this vaccine is a milestone as we continue to battle the COVID-19 pandemic. While this and other vaccines have met the FDA’s rigorous, scientific standards for emergency use authorization, as the first FDA-approved COVID-19 vaccine, the public can be very confident that this vaccine meets the high standards for safety, effectiveness, and manufacturing quality the FDA requires of an approved product.”
The very next day, the U.S. Defense Secretary, Lloyd Austin, issued a memorandum mandating the COVID-19 vaccine for all military service members.
Woodcock’s claim that the Pfizer/BioNTech mRNA vaccine met “the FDA’s rigorous, scientific standards for Emergency Use Authorization,” granted on December 11, 2020, is paradoxical considering the less stringent nature of the EUA process.
For instance, in times of a public health emergency or crisis, investigational medical countermeasures can be authorized under an Emergency Use Authorization (EUA) mechanism without complete clinical trial data. In addition, the FDA can grant an EUA of an investigational vaccine on the vague notion that it may be effective, and that its known and potential benefits outweigh its known and potential risks.
The anomalies of the FDA’s October 2020 meeting
In the lead-up to the EUA, a public meeting of the FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) was convened on October 22, 2020, to deliberate on the development, authorization, and/or licensure of vaccines intended to prevent COVID-19.’ Ironically, Phase III COVID-19 vaccine trials were never designed to prevent transmission of COVID-19 or measure reductions in serious outcomes, like hospitalizations and death. This critical aspect was completely overlooked in the FDA’s deliberations.
From the start of the COVID-19 vaccine rollout, government officials, public health authorities, and mainstream media engaged in a concerted effort to disseminate misinformation by claiming that COVID-19 vaccines “stop the spread,” despite them never being designed to prevent transmission.
During the meeting, Dr. Peter Marks, FDA Chief of the Center for Biologics Evaluation and Research, chose to remain silent on that issue. However, four years later, during a hearing of the Select Subcommittee on the Coronavirus Pandemic, Dr. Marks confessed when queried by Rep. Michael Cloud about whether the “COVID-19 vaccines stop transmission,” he acknowledged, “it does not absolutely prevent transmission.”
The “smoking gun” vaccine adverse event presentation slide
Another striking anomaly emerged during the 9-hour meeting: the brief glimpse of a bombshell FDA vaccine safety slide that seemed to go unnoticed. This damning slide, which flashed for only a moment was part of Steven Anderson’s presentation, the FDA’s Director of the Office of Biostatistics and Pharmacovigilance, on the Centre of Biologics Evaluation and Research (CBER)’s plans for monitoring COVID-19 vaccine safety and effectiveness.
The ‘FDA Safety Surveillance of COVID-19 Vaccines’ presentation slide appeared on the screen at the 2:33:40 timestamp. This “smoking gun” slide listed an extensive catalogue of possible adverse event outcomes associated with COVID-19 vaccines, known by the FDA as early as October 2020, long before EUA was granted by the agency.
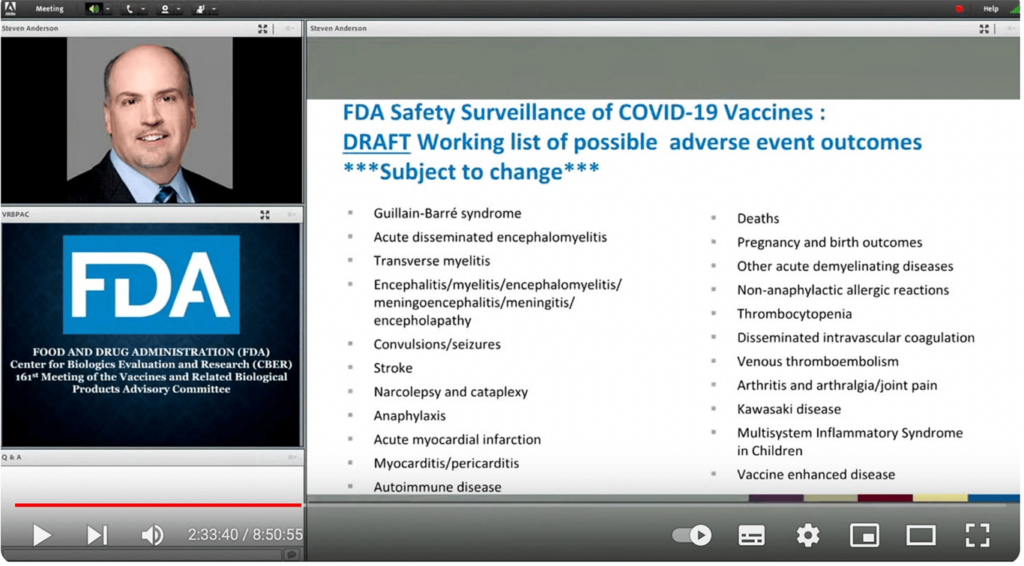
The only reference made to the slide is where Anderson states, “Tom [Tom Shimabukuro] has a list of possible adverse outcomes of interest. I won’t dwell on this..”
Indeed, Anderson did not dwell on it, as evidenced by the slide’s brief appearance. This indicates that there was no intention to discuss or emphasize the content of the slide; rather, it seems that the FDA sought to bury its significance by quickly moving on from it.
The catalogue of adverse events
The extensive list of serious possible adverse event outcomes “subject to change,” known by the FDA around two months before EUA was granted, is highly noteworthy.
Firstly, none of these possible serious adverse events were included in any of the initial packaging inserts of the investigational products. Official news of the risk of myocarditis/pericarditis for young adolescent males first broke around April 2021– months after the mRNA shots were distributed. It is deeply concerning how the FDA proceeded to expand authorisation of these experimental mRNA products for those aged 12 through to 15 years, just a month later, on May 10, 2021, when evidence of the risk of this serious condition was identified (in their own presentation slide) by the agency as early as October 2020.
The FDA’s list of adverse events, labelled as “subject to change,” has indeed proven accurate, as it has expanded considerably since that October 2020 meeting.
My early analysis of Pfizer’s 38-page document, entitled, “Cumulative Analysis of Post-Authorization Adverse Event Reports of PF-07302048 (BNT162B2) received through 28 February 2021” for Trial Site News in December 2021, showed that in the first 3-month period, post authorization, 1228 deaths had been reported along with an 8-page list of adverse events of special interest.
A further revelatory document discovered among the trove of court-ordered released Pfizer papers, was the pharmaceutical behemoth’s Pregnancy & Lactation Cumulative Review, which I unearthed and reported on for Trial Site News. These critical documents were intentionally concealed by the FDA, with the aim of keeping them hidden from public view until 2096.
The cumulative review of pregnancy and lactating cases was sourced from Pfizer’s pharmacovigilance (safety) databases spanning from the time of drug development through to February 28, 2021. Out of the 458 pregnancy cases, a staggering 248 (more than half) reported adverse events. Despite this alarming data, the CDC proceeded to recommend the experimental gene therapy product to pregnant mothers. This recommendation came just three days after the review was signed off on April 20, 2021, and submitted to the FDA.
Despite assurances that Emergency Use Authorizations (EUAs) for Moderna and Pfizer/BioNTech’s experimental gene therapy products were granted with rigorous ongoing safety surveillance post-authorization, mounting evidence of harms captured on safety surveillance systems worldwide and buried in FOIA-released documents did not prompt a revocation of their EUAs. Instead, they were ultimately approved and licensed. Perhaps, echoing Woodcock’s own words, this was done to ensure that “the public can be very confident that this vaccine meets the high standards for safety, effectiveness, and manufacturing quality the FDA requires of an approved product.”
The vaccine safety study on 99 million individuals
In February of this year, the largest global study of its kind on 99 million vaccine recipients across eight countries, was published in Vaccine, linking increases in heart, blood and neurological disorders to the Pfizer, Moderna and Astra Zeneca COVID-19 shots.
This study by Faksova et al. confirmed previously identified safety signals for myocarditis and pericarditis after Pfizer and Moderna’s mRNA vaccines and Guillain-Barré syndrome and cerebral venous sinus thrombosis after AstraZeneca’s viral vector vaccine- also included in the FDA’s October 2020 presentation slide.
According to a report in The British Medical Journal: ‘this vaccine safety study [Faksova et al.] to date has identified two new, but very rare, side effects associated with covid-19 vaccines—transverse myelitis and acute disseminated encephalomyelitis.’
However, what is particularly alarming is that both transverse myelitis and encephalomyelitis, the two side effects mentioned, are not new. They were included as possible adverse event outcomes of the COVID-19 vaccines in the FDA’s October 2020 presentation slide.
The v-safe text data hidden by the CDC
Another speaker, who presented during the FDA meeting was Dr Tom Shimabukuro of the CDC COVID-19 vaccine Task Force, (referred to later by Anderson) who addressed the group on CDC post-authorization/post-licensure safety monitoring, including the use of Vaccine Adverse Event Reporting System (VAERS), Vaccine Safety Data link (VSD) and the launch of the new V-safe program.
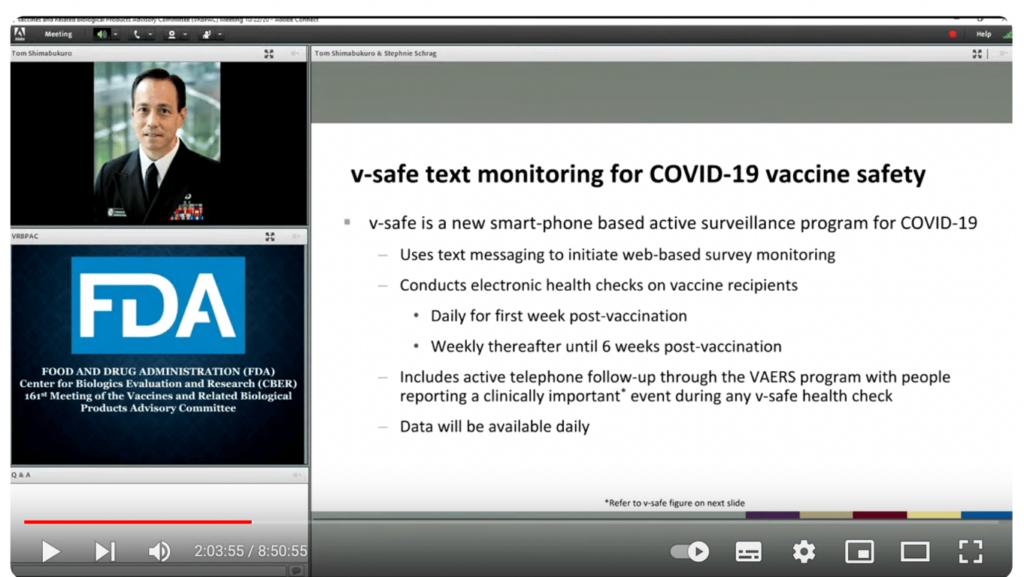
Dr Shimabukuro discussed how the CDC’s pivotal V-safe, a smartphone-based active surveillance program, would use text messaging to initiate web-based survey monitoring after Covid-19 vaccination. He made a point of stating how the “data will be available daily.”
Approximately 10 million people signed-up and submitted health reports after Covid-19 vaccination, none of the data was made available daily- in fact, it was never released at all.
The ICAN’s legal team sued the CDC twice to obtain the data, which led to a court-order requiring the release of it. It took until February this year for ICAN to receive the first production of the V-safe free text data.
In an interview with Del Bigtree, Aaron Siri, legal counsel of the ICAN legal team said: “A federal judge in an incredible 29-page decision has now issued an order requiring the CDC to make every single one of those 7.8 million free text entries available to the public over the next twelve months. Every month they have to produce a few hundred thousand of them…It will be an incredible opportunity to actually see what was being told to the CDC by the public…I think this is going be the death blow to this cover-up. It is clear that they’ve been hiding something and now the world is about to see what people wrote in after getting the vaccine.”
The screenshot below shows a breakdown of the CDC data sourced by ICAN.

Out of the 10,108,273 users, roughly a third were impacted by adverse health.
Turning back to the February 15, 2024, hearing of the Select Subcommittee on the Coronavirus Pandemic, Chairman Dr Brad Wenstrup asked Dr Peter Marks the following question: “As of February 2024, Vaccine Adverse Event Reporting System (VAERS) reports for COVID-19 vaccines total significantly higher than all other vaccines combined since 1990. This is a surprising figure. Dr Marks, was the government prepared for such an avalanche of reports to VAERS?”
Dr Peter Marks: “We tried to be prepared for that, but the avalanche of reports was tremendous. It, again, required re-tasking people on the fly…We had to usually staff up and had many meetings working to increase our ability to go through these reports.”
Marks also admitted “we probably have not done a good enough job” accurately informing Americans about confirmed COVID-19 vaccine deaths and injuries.
It is evident that both the FDA and CDC have failed in their obligations to safeguard the health of Americans. Likewise, regulators worldwide have also fallen short in protecting their citizens. However, what is truly reprehensible is the intentional effort to conceal the damning data on adverse events, especially considering that these risks were known before a single shot was administered to the unsuspecting public, who were never provided with informed consent.
Suggest a correction


